WHAT IS GUNN IMS?
Intramuscular Stimulation (IMS) is a total system for the diagnosis and treatment of myofascial pain syndromes (chronic pain conditions that occur in the musculoskeletal system when there is no obvious sign of injury or inflammation). Gunn IMS is a specialized physiotherapy service that PRI provides to our patients. It requires practitioners to have extensive physiotherapy experience before being admitted to training.
HOW DOES IMS WORK?
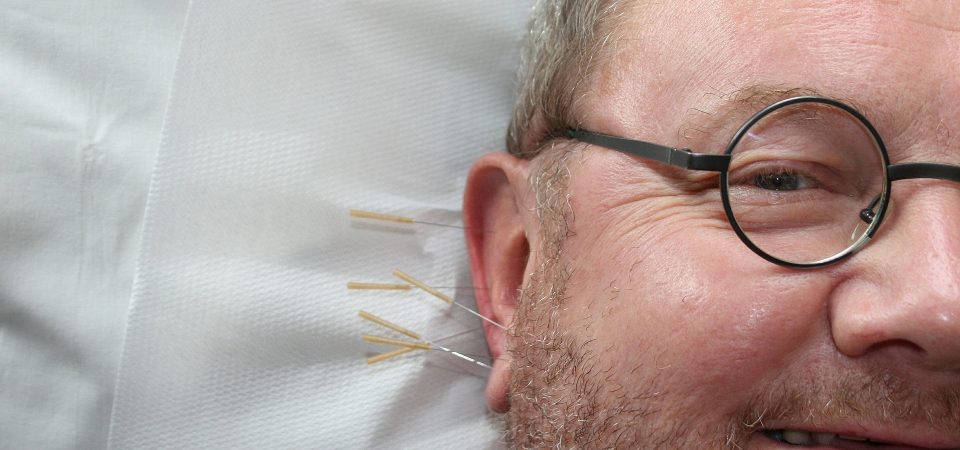
IMS is grounded in Western Medical Science, and uses acupuncture needles that are designed to penetrate deep within muscle tissue, specifically targeting injured muscles that have contracted and become shortened from distress.
IMS TREATMENT DESCRIPTION
IMS therapy relies heavily on a thorough physical examination of the patient by a competent practitioner, trained to recognize the physical signs of neuropathic pain. This physical examination is indispensable since chronic pain is often neurological as opposed to structural, and therefore, invisible to expensive X-rays, MRI Tests, Bone and CT Scans. Failure to recognize these signs will result in an inaccurate diagnosis, and thus, a poor starting point for physical therapy. The treatment involves dry needling of affected areas of the body without injecting any substance. The needle sites can be at the epicenter of taut, tender muscle bands, or they can be near the spine where the nerve root may have become irritated and supersensitive. Penetration of a normal muscle is painless; however, a shortened, supersensitive muscle will ‘grasp’ the needle in what can be described as a cramping sensation. The result is threefold. One, a stretch receptor in the muscle is stimulated, producing a reflex relaxation (lengthening). Two, the needle also causes a small injury that draws blood to the area, initiating the natural healing process. Three, the treatment creates an electrical potential in the muscle to make the nerve function normally again. The needle used in IMS, by stimulating muscle spindles, essentially becomes a specific and unique tool for the diagnosis of Neuropathic Muscle Pain.
CAN YOU SHOW ME HOW THE SPINE MAY BE INVOLVED?
The most common cause of nerve irritation and neuropathic pain is “spondylosis,” degeneration of the spine, which can result from normal wear and tear. Spondylosis irritates the nerve root and leads to neuropathy and muscle shortening.
WHAT IS THE GOAL IN USING IMS?
The goal of treatment is to release muscle shortening, which presses on and irritates the nerve. Supersensitive areas can be desensitized, and the persistent pull of shortened muscles can be released. IMS is very effective for releasing shortened muscles under contracture, thereby causing mechanical pain from muscle pull. IMS, in effect, treats the underlying neuropathic condition that causes the pain. When competently performed, IMS has a remarkable success rate, as proven by the amelioration of symptoms and signs, even for chronic back pain with root signs.
HOW OFTEN SHOULD I HAVE IMS?
Treatments are usually once a week to allow time between treatments for the body to heal itself. The number of treatments you require will depend on several factors such as:
1. the duration and extent of your condition
2. how much scar tissue there is, (usually increased after previous surgery)
3. how quickly your body can heal depending on the condition of your nerves.
If the pain is of recent origin, one ims treatment may be all that is necessary. In published studies of patients with low back pain, the average number of IMS treatments required was 8.2.
IS IMS THE SAME AS ACUPUNCTURE?
IMS is comparable in some ways to acupuncture; however, there are a number of important differences. IMS requires a medical examination and diagnosis by a practitioner knowledgeable in anatomy, needles insertions are indicated by physical signs and not according to predefined, non-scientific meridians, while subjective and objective effects are usually experienced immediately.
If you have been injured athletically, at work or in an automobile accident and haven’t had success with traditional types of treatment, IMS may be worth trying.